 The two minute talks
The two minute talks this week were based around “the use of...” various drugs. I hope that these have stimulated some thought....and curiosity about other drugs you use regularly. It is important as you continue in your training to give increasing thought to the reasons and evidence behind the guidelines and advice associated with drugs.
Gentamicin: (SS) a drug with a narrow therapeutic window. Various methods exist for monitoring gentamicin levels. The aim is to give the correct dose (to achieve levels high enough for effect and low enough to be safe). It is because dose calculations do not always predict the correct dose that levels must be monitored to allow fine tuning of dose and frquency.
Thrombolytics (HJ) nostalgia prompted my question about fibrinolytics (apologies). Another drug with significant risks to balance against benefits. Before PCI was easily available the decision for patients with a relative contra-indication was thrombolyse or nothing and greater risks may have been accepted than would now be appropriate.
Amiodarone (JB) the ‘greedy’ anti-arrythmic with a bit of each class activity, broad spectrum activity and plenty of drawbacks. Time to review the Vaughn Williams Classification, but before you do revise, the cardiac action potential. I used to find it difficult to understand the why particular drug classes had their effects until tied them in with the action potential and the fact, that escaped me for years, that the fast depolarisation channel in the SA node and AV node is calcium rather sodium mediated.
Heparin (R) I hold my head in shame. I did not know that heparin could produce hyperkalaemia yet the Oxford textbook says hyperkalaemia occurs in 7% of heparin treated patients due to inhibition of aldosterone production. I will be on the look out now.
Warfarin (HA) I now know that vitamin K is named for Koagulation. You now know why we need to continue heparin for a couple of days after the INR is therapeutic. That pesky protein C.
For next week you are excused the two minute tutorials but sentenced to the three minute tests. You will be asked to give the initial management of an emergency. There aren’t that many possibilities, so get revising.
The paper discussed on Tuesday was
Thoughts for new medical students at a new medical school, Richard Smith. By the way, have you read his articles about Dumfries? How about leaving your advice for newly appointed house officers in the comments? I’ll post it with your photo in the
hall of fame if you like.
For next Tuesday I would like you to read
In a stew. Michael A Lacombe. American Journal of Medicine. 1991;91:276-278. If you feel up to it, read the associated editorial
Double trouble, boil and bubble. And ask yourself how I came across these articles in a journal I do not regularly read.
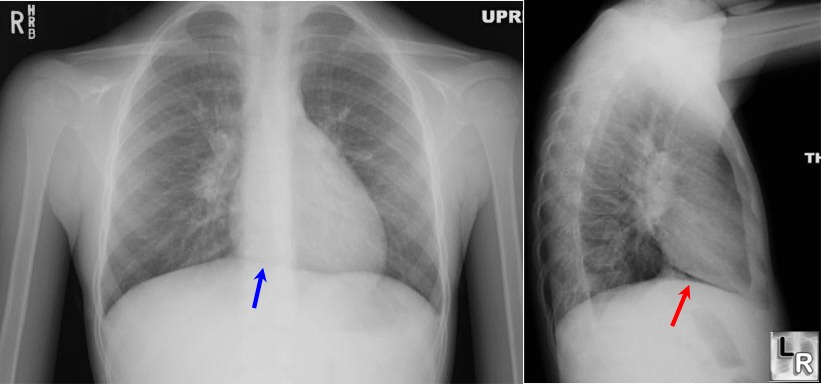
Interesting TopicsPneumomediastinum See also
this link which explains the X-ray above.
MJM


























{kind=link}
{kind=link}